Funny that my last post ended with talking about planning meals. On Friday (as Rich says, “Why always Fridays?”) I came down from my remote office for lunch and found Rich leaning forward fast asleep. While napping is innocuous, his position was not. Any time I see that posture, it’s a good indicator that we’re in for a bit of a ride.
I woke him up and we chatted for a bit about lunch and then segued onto a discussion on our plans for dinner. As we got up to check the freezer and make some decisions, Rich was a little off balance. It happens. So, we wait for his BP to stabilize from the change in altitude. Called orthostatic hypotension or positional hypotension, Rich is used to this and generally will take a moment when getting up from a chair to allow everything to equalize. Walking behind him as we made our way through the house, I could see he was lightly touching the furniture he passed to orient himself upright. Not a good sign.
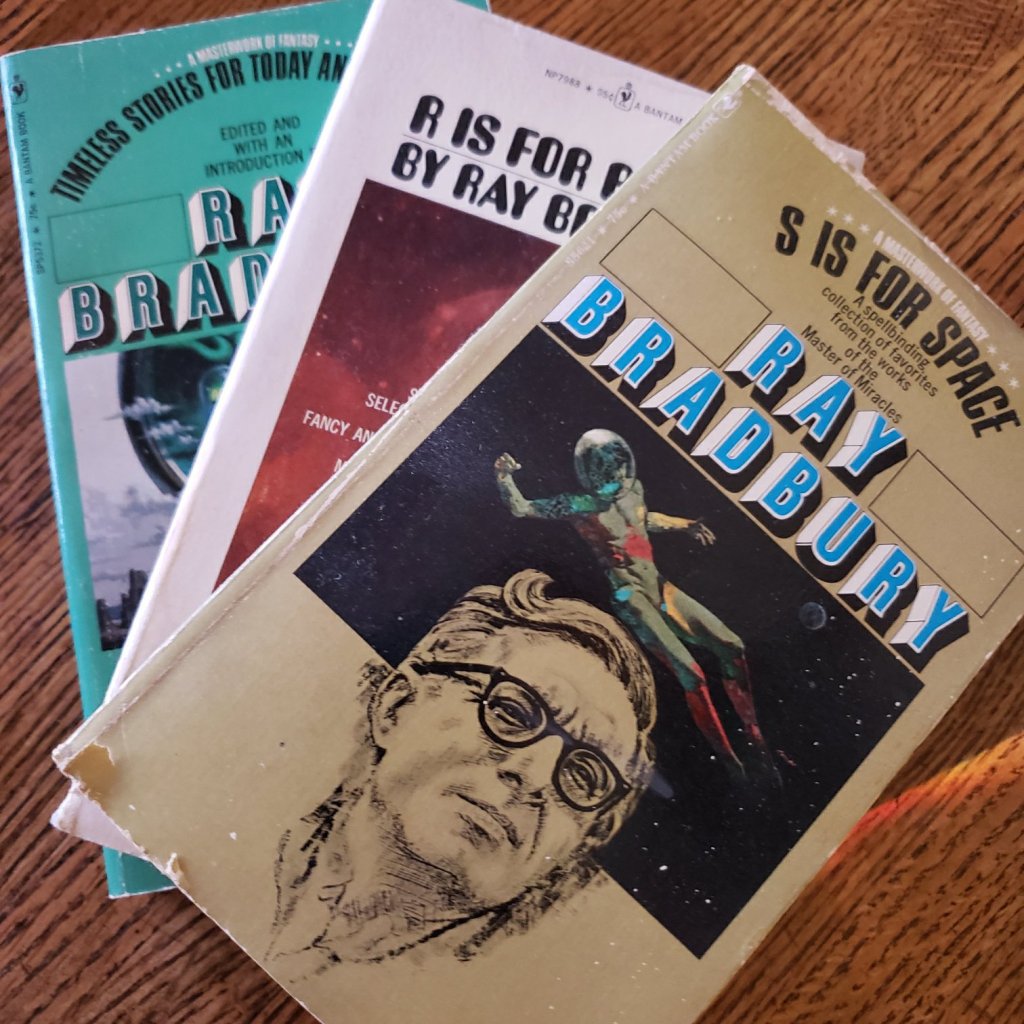
Before I knew it, his eyes rolled back, and he began to crumble into himself. Syncope. While trying to catch him, I also pushed him up against the nearby bookcases to help me keep him from hitting sharp corners until I could get myself under his arm properly to support him. With the canon of Ray Bradbury practically up his nose and his nose on the shelf pretty much all that was keeping him from crashing down, I kept saying his name louder and louder to bring him back to consciousness. He’s not a small guy and I needed more than some dead weight to keep him from some serious damage. In his confusion when he began to become aware again, he kept saying he was fine. Fine. Nose hooked onto a bookshelf filled with the yellowing seventy-five cent mass markets of Bradbury’s nostalgic science fiction. Truthfully, there are worse places to be.
Once settled, Rich’s blood pressure seemed elusive. Finally, some readings start to show we’re in low blood pressure territory again. Since his last hospitalization, we’ve had a few of these episodes but with some additional fluids and rest, we’ve been able to bring it back up to the norm. Now was not one of those times. When we finally got a reading, it was 78/45. A call to the heart failure doctor’s office confirmed a trip to the ER was needed.
Once again, with covid protocols in place, I dropped Rich off in a way that felt very much like dropping off some dry cleaning… albeit some with some pesky stains that needed special attention.
As they ran tests, they inverted Rich to keep his brain well supplied with blood. Through some trial and error to get needed data, they took his BP lying down, sitting up and standing. Lying down and standing up our guy was in normal range. But sitting, SITTING, his BP dropped to a low of 70/43. None of this made any kind of sense.
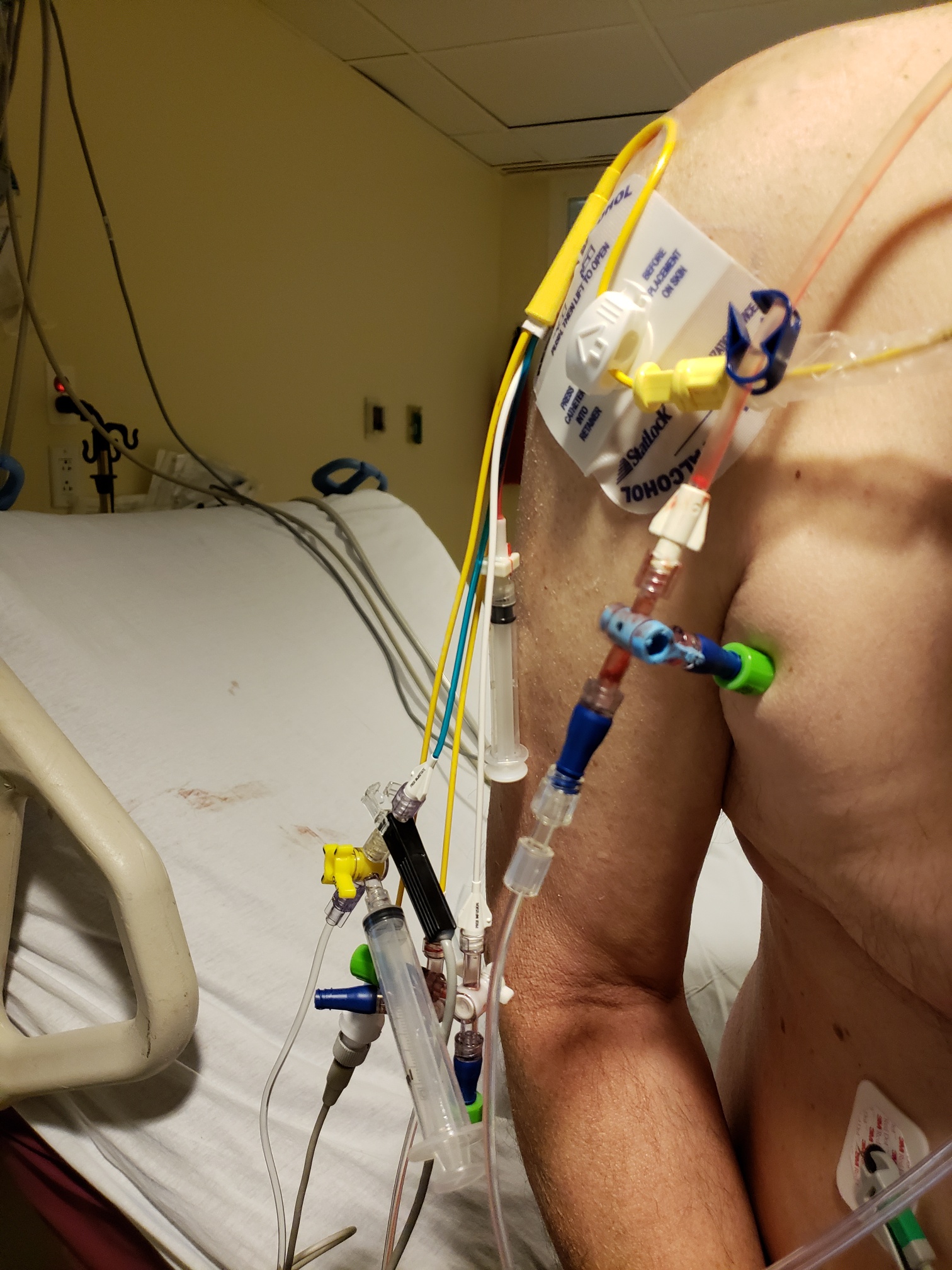
Saturday morning, they ran some blood work specific to heart related issues. These were tests that we’ve never seen before, but we do know that the doctors were looking for any kind of infections that would preclude surgery. Because it looks like Rich’s CRT-D implantation into the Borg collective was getting moved up.
In addition to this expected device, we’re also advised that there is another device that is being considered in addition to the pacemaker/defibrillator. This one is called a Cardiomem. This little piece of magic measures pressure in and around the heart to help control medications having to do with the congestive part of congestive heart failure. By measuring that pressure, it is measuring the indication of fluid buildup before our patient has any sense of water retention or bloating. As it’s constantly monitoring and in communication with the health care community, we can be advised to begin taking lasix to forestall any buildup that can be problematic.
Our consults are via phone; Rich and the doctors in his hospital room on one end, and me at home on the other. The waiting, never my strong suit, is maddening. I’m allowed to visit now that some covid restrictions are lifted. I wait on a long line of visitors. My temperature is taken. A timed visitor badge is given to me. I’m told my visit is limited to two hours.
I’m supposed to check in at the nurse’s station in Rich’s unit. I bypass that protocol, I really don’t want a record of when I came in. I stay for eight hours. At one point, six hours have passed, and I ask Rich’s nurse when she will kick me out. She looks at me and meets my eyes. “I don’t think you want to ask me that.” Got it.
At the end of hospital-wide visiting hours, I leave. There will be no overnight stays yet. We had hoped a doctor would be stopping by while I was there, but the room has been quiet as we binged our current TV show. We treasure the time.

Sunday morning the latest news is that electrophysiology is working to schedule Rich for his CRT-D device on Monday at the earliest. After I hang up from the teleconference, the house is once again too quiet. As is my norm, I turn to music to fill the emptiness and the first of the mix is an earworm that has been stuck in my head these last couple of days. A duo from Ireland that we’ve followed from their days in the The Choral Scholars of University College Dublin. It feels like they’ve been along with us on our CHF journey where we kept insisting in 2018: we have a trip planned to Ireland, we’re going. Their harmonies soothe and, as always, lift us at those moments when we need our spirits to soar beyond the now.
And yes, soon, it will be time for Rich to come home. Not yet, but soon. Because there’s someone I’ve been missing. Who is the better half of me.
Thank you to glenn&ronan for this cover of Come Home.
Hello world
Hope you’re listening
Forgive me if I’m young
For speaking out of turn
There’s someone I’ve been missing
I think that they could be
The better half of me
They’re in the in the wrong place trying to make it right
But I’m tired of justifying
So I say to you
Come home
Come home
‘Cause I’ve been waiting for you
For so long
For so long
And right now there’s a war between the vanities
But all I see is you and me
The fight for you is all I’ve ever known
So come home
I get lost in the beauty
Of everything I see
The world ain’t as half as bad
As they paint it to be
If all the sons
If all the daughters
Stopped to take it in
Well hopefully the pain subsides and the love can begin
It might start now
Well maybe I’m just dreaming out loud
Until then
Come home
Come home
‘Cause I’ve been waiting for you
For so long
For so long
And right now there’s a war between the vanities
But all I see is you and me
The fight for you is all I’ve ever known
So come home
Everything I can’t be
Is everything you should be
And that’s why I need you here
Everything I can’t be
Is everything you should be
And that’s why I need you here
So hear this now
Come home
Come home
‘Cause I’ve been waiting for you
For so long
For so long
And right now there’s a war between the vanities
But all I see is you and me
The fight for you is all I’ve ever known
So come home